Superior Labrum SLAP
“SLAP tear” refers to a specific injury of the superior portion of the labrum at the glenoid socket of the shoulder. The original description refers to an observed pattern of injury to this portion of the labrum that runs from anterior to posterior(1). There was a pattern of the occurrence of these lesions in overhead athletes and laborers performing routine overhead activities. The diagnosis of a SLAP tear is based on both clinical, imaging, and arthroscopic information. Not all labral detachments at this location of the shoulder require specific intervention as there is a wide variety of normal anatomic variability in the general population and these lesions can occur coincidentally with other diagnoses, including rotator cuff disease.
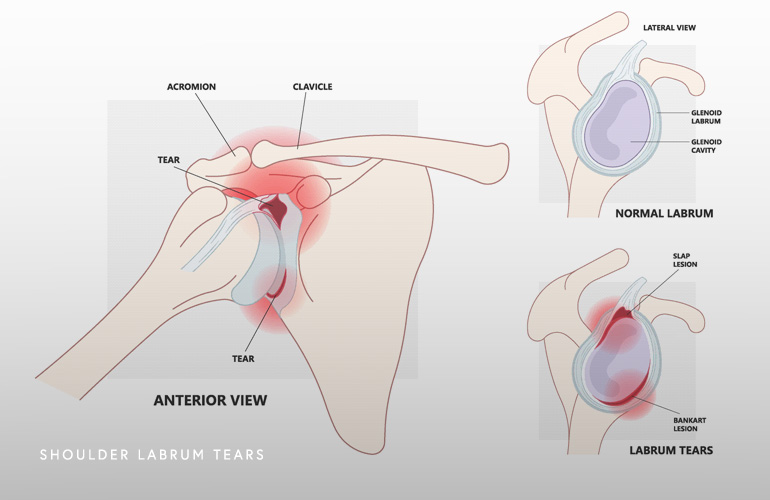
The labrum is a fibrocartilaginous (spongy) ring that attaches to the outer glenoid (socket) rim, serving to increase the area of contact between the humeral head and glenoid and provides additional depth to the glenoid. This increased contact area stabilizes the shoulder joint which permits the shoulder to enjoy a profound range of motion in many planes without increasing the areas of bony constraint. Also importantly, the labrum serves as the attachment point of the ligaments of the shoulder as well as the long head of the biceps tendon.
When thinking about the etiology of SLAP tears, it is helpful to think about these tears as either traumatic or degenerative, which affects treatment decisions. One of the more common mechanisms for traumatic injury to the superior labrum involves forceful eccentric traction on the labrum through the biceps tendon as when someone falls back onto an outstretched arm or when suddenly jerking the shoulder as when lifting a heavy object. Another way the biceps can injure the labrum at this location involves the patient grabbing an object such as a handrail or ledge when falling. Dislocation events of the shoulder can similarly cause an eccentric pull through the biceps tendon that generates a tear of the superior labrum.
SLAP lesions can also occur in throwing athletes or individuals with repetitive overhead occupational demands when the shoulder is abducted and externally rotated (as when throwing a ball or swinging a hammer). During the cocking phase of throwing, the humeral head generates shear forces superiorly in the glenoid which is resisted by the superior labrum and anterior joint capsule, generating a load that can cause gradual tearing and injury to the superior labrum. This mechanism is called “peel-back” and can be observed at arthroscopy in throwing athletes. Further contributing to this mechanism in throwers is the continued pull from the biceps tendon that causes an avulsion of the superior labrum.
Also relevant to throwing athletes, the hyper-external rotation seen in elite pitchers causes a compensation in the ligaments (capsule) changes the available arc of motion externally for throwing while diminishing the amount of internal rotation. This phenomenon can lead to inflammation and later contracture of the posterior capsule called “GIRD” (glenohumeral internal rotation deficit), leading to a condition referred to as “internal impingement” and can become painful and lead to SLAP tearing. Also characteristic of this process is undersurface tears of the rotator cuff.
Lastly, the degenerative variety of SLAP tears, which are most common, occur with a wear-and-tear mechanism and are felt to occur through a gradual increased superior translation of the humeral head as when a tear or injury occurs at the rotator cuff. The humeral head gradually pushes up into the labrum, generating microtrauma and tearing at that location. Contractures of the posterior capsule also contribute to superior humeral head translation and SLAP tearing. These degenerative tears are important to identify as the treatment is different for traumatic SLAP tears.
The symptoms of SLAP tears are often vague and sometimes confused with symptoms occurring from other concomitant sources, as from the rotator cuff. Anterior shoulder pain may occur and the athlete or laborer may complain of clicking or catching as when the arm is in the cocking position of throwing. Patients with a traumatic injury such as a glenohumeral dislocation reporting continued anterior or deep shoulder pain sometimes can be cause by a SLAP tear. Despite these clues, there is no consistent activity of daily living that causes pain and the diagnosis is confirmed with the combination of the physical examination and the results of imaging.
Typically, a period of nonsurgical treatment is initiated with a period of avoidance of painful arm positions such as throwing or overhead work, and a structured rehabilitative program emphasizing improving the kinetics of the scapula and stretching the posterior capsule which is associated with glenohumeral rotation deficits. Rotator cuff strengthening is also an important component of the rehabilitative program. Injections can be used to modulate inflammation and provide pain relief during the initiation of a structured exercise program.
In patient who fail nonsurgical management, arthroscopic surgery may be warranted. In patients with isolated SLAP tears, depending on concomitant pathology, sometimes the SLAP tear alone can be repaired with a bioabsorbable knotless implant that provides long term fixation and obviates concern for irritation from knots and prominent implants in the joint. Often times, SLAP repair can be performed with a biceps tenodesis to stop the eccentric pull from the biceps, which can lead to pain and stiffness if not performed. Older patients presenting with rotator cuff and other lesions are frequently treated with debridement of the SLAP tear and biceps tenodesis, as clinical outcomes have increasingly supported this treatment algorithm amongst experienced shoulder surgeon like Dr. Obermeyer(2).
Schedule an orthopedic appointment
If you have symptoms consistent with SLAP tear, call our office or book an appointment with shoulder surgeon Dr. Thomas Obermeyer. Dr. Obermeyer specializes in diagnosing and treating shoulder injuries. Dr. Obermeyer has orthopedic offices in Schaumburg, Bartlett, and Elk Grove Village, Illinois. Dr. Obermeyer regularly sees patients from throughout Illinois including Hoffman Estates, Palatine, Elgin, Streamwood, Arlington Heights, and Roselle communities.
References
- Snyder SJ, Karzel RP, Del Pizzo W, Ferkel RD, Friedman MJ. SLAP lesions of the shoulder. Arthroscopy. 1990;6(4):274-9. doi: 10.1016/0749-8063(90)90056-j. PMID: 2264894.
- Abbot AE, Li X, Busconi BD. Arthroscopic treatment of concomitant superior labral anterior posterior (SLAP) lesions and rotator cuff tears in patients over the age of 45 years. Am J Sports Med. 2009 Jul;37(7):1358-62. doi: 10.1177/0363546509331940. Epub 2009 Apr 13. PMID: 19364887.
At a Glance
Dr. Thomas Obermeyer
- 15+ years of training and experience treating complex shoulder and sports medicine conditions
- Expert subspecialized and board-certified orthopedic care
- Award-winning outstanding patient satisfaction scores
- Learn more
