Posterior Instability and Posterior Labral Tears
What is Posterior Instability?
Posterior instability of the shoulder is a condition where the ball of the shoulder injures tissues towards the back (posterior) part of the socket. This can occur as a single traumatic event after an injury or can occur as a result of repetitive “microtrauma” where the culmination of daily activities or sporting demands that ordinarily would be well tolerated can lead to pain and dysfunction. Posterior instability is increasingly recognized as a diagnostic challenge(1) because of the frequent insidious nature of the symptoms, the often subtle imaging findings on MRI, and the subtleties of physical examination that are key to diagnosis. Unlike anterior instability where there frequently is a clear traumatic event such as a dislocation, posterior instability symptoms sometimes may not have that history and only manifest as pain. Oftentimes, the astute clinician can diagnose posterior instability after a detailed history and physical examination, with MRI serving as a confirmatory test and to screen for associated conditions.
The bony anatomy of the shoulder is inherently incapable of holding the joint in position through an arc of motion without the soft tissue stabilizers, including the ligaments and the bumper of cartilage called the labrum. This is because the socket bone is very shallow and flat, and by itself provides little in the way of supporting “congruency” (holding) of the ball during arm function. In the case of posterior instability, activities that place the arm in front of the body (such as reaching directly forward or across the body) place forces that tend to cause the ball to push out the back of the socket. Some patients have loose ligaments and tissues as part of their normal anatomy to begin with and this laxity leads to subtle instability events where the ball can slide out the back of the socket(2). In these patients, the instability is very minimal and requires many repetitions of a sporting activity to cause a problem, and in other patients, the shoulder has normal anatomy but sustains a single traumatic event with the arm in front of the body (as in a football lineman blocking an opposing player) which causes an injury. In either case, a particular band of the capsular ligaments called the posterior inferior glenohumeral ligament is typically loosened with posterior instability, along with a tear in the posterior labrum(3).
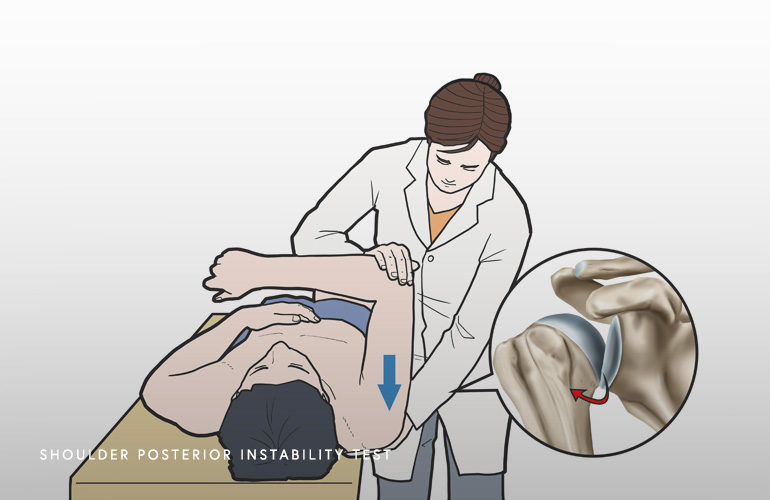
A careful history and physical examination is critical for the diagnosis of posterior instability. This condition can affect patients of all ages but is characteristically seen in young athletic patients often without a history of a single traumatic event. As noted above, the tears in the posterior labrum in posterior instability are often small and subtle and sometimes missed by radiologists and clinicians. A diagnostic clue is pain that is deep and sometimes radiating in the shoulder blade or in the arm, worse with activity. The physical examination also is important, and provocation of the shoulder with the patient lying back on an exam table is necessary, as well as evaluation of ligamentous laxity which is a common finding in patients with posterior instability.
In patients that have sustained a traumatic event, MRI is usually more evident with a more clearly visualized (displaced) tear, sometimes with a bony chip in the bone (called a reverse Bankart lesion) or with a dent in the ball called a reverse Hill-Sachs Lesion. These more significant bone injuries can also be seen in patients with epilepsy, where a seizure causes the muscles to involuntarily dislocate the ball of the shoulder. In patients suspected of having posterior instability, it is helpful to undergo MRI scanning with a contrast material injected into the shoulder before the test to improve the visualization of subtle tears in the labrum that otherwise would be difficult to see. Ultimately, the gold standard diagnosis is arthroscopic surgery, where the labral tissue can be probed and the shoulder examined while visualizing the tissue directly.
The treatment decision for posterior instability is dependent on the chronicity and severity of symptoms, imaging findings, and demands of the patient. Athletes who develop pain mid-season during competitive sporting may consider a period of activity modification where the painful arm positions are limited for a time, followed by a course of physical therapy to strengthen the rotator cuff and shoulder blade muscles. Strengthening the subscapularis, which is a powerful muscle in the front of the shoulder and helps to counteract posterior shifting of the joint, is a helpful exercise goal. In patients that have hyperlaxity, initiating a course of physical therapy is often recommended.
In athletes with ongoing pain despite conservative treatment, who are in the offseason, or who have clear structural labral and capsular tearing such as after an injury, arthroscopic surgery is recommended. The goals of arthroscopic surgery are to alleviate pain from the torn and damaged labrum bumper and to tension the capsule/ligaments appropriately, to prevent reinjury and to rebalance the ligaments in the back of the shoulder. This tissue (the posterior inferior glenohumeral ligament) is tensioned and repaired with arthroscopic techniques. The methods and sutures used for arthroscopic soft tissue repair are much lower profile, do not rely on irritating knots in the shoulder joint, and have excellent purchase and fixation in comparison with prior generations of arthroscopic technology.
Schedule an orthopedic appointment
If you have symptoms consistent with posterior instability, call our office or book an appointment with shoulder surgeon Dr. Thomas Obermeyer. Dr. Obermeyer specializes in diagnosing and treating shoulder injuries. Dr. Obermeyer has orthopedic offices in Schaumburg, Bartlett, and Elk Grove Village, Illinois. Dr. Obermeyer regularly sees patients from throughout Illinois including Hoffman Estates, Palatine, Elgin, Streamwood, Arlington Heights, and Roselle communities.
- Provencher MT, LeClere LE, King S, McDonald LS, Frank RM, Mologne TS, Ghodadra NS, Romeo AA. Posterior instability of the shoulder: diagnosis and management. Am J Sports Med. 2011 Apr;39(4):874-86. doi: 10.1177/0363546510384232. Epub 2010 Dec 4. PMID: 21131678.
- Dewing CB, McCormick F, Bell SJ, Solomon DJ, Stanley M, Rooney TB, Provencher MT. An analysis of capsular area in patients with anterior, posterior, and multidirectional shoulder instability. Am J Sports Med. 2008 Mar;36(3):515-22. doi: 10.1177/0363546507311603. Epub 2008 Jan 23. PMID: 18216272.
- Kim SH, Ha KI, Park JH, Kim YM, Lee YS, Lee JY, Yoo JC. Arthroscopic posterior labral repair and capsular shift for traumatic unidirectional recurrent posterior subluxation of the shoulder. J Bone Joint Surg Am. 2003 Aug;85(8):1479-87. doi: 10.2106/00004623-200308000-00008. PMID: 12925627.
At a Glance
Dr. Thomas Obermeyer
- 15+ years of training and experience treating complex shoulder and sports medicine conditions
- Expert subspecialized and board-certified orthopedic care
- Award-winning outstanding patient satisfaction scores
- Learn more
