Lateral Epicondylitis
What is lateral epicondylitis?
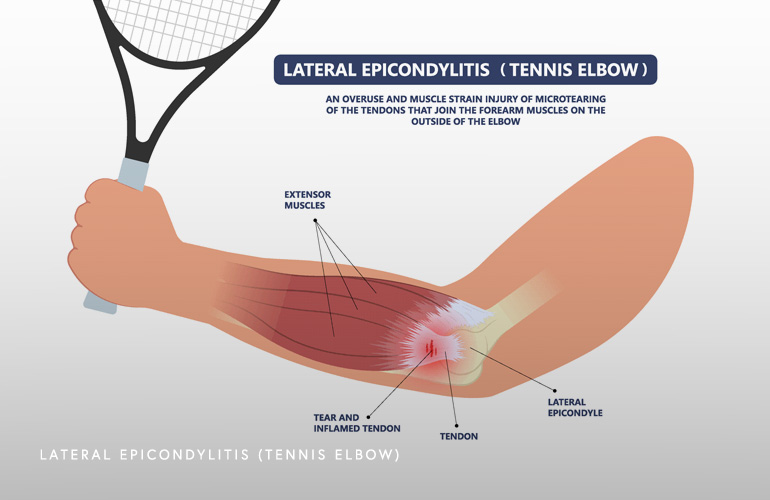
Lateral epicondylitis refers to the anatomical location of pain that develops as a result of chronic overuse (or sometimes acute injury) to the tissue at the lateral (outer) portion of the elbow. Structurally, the tendon that is activated with forceful gripping at the outer elbow called the extensor carpi radialis brevis (and to a lesser extent the extensor digitorum communis) leads to an injury causing pain and tenderness to the touch at the bony outer tip of the elbow called the lateral epicondyle. Because of the high degree of load transmitted through this very tendon with repetitive activities such as gripping a tennis racket, the condition has been coined the “tennis elbow”. Indeed, lateral epicondylitis is commonly seen in tennis players, but can occur in non-athletes, golfers, and in injured workers(1).
While there are certain incompletely understood features about the pathophysiology (underlying problem leading to the condition) of lateral epicondylitis, it is believed either a repetitive or acute trauma to the outer tendon of the elbow leads to characteristic findings when the tissue is inspected under a microscope. The term “angiofibroblastic tendinosis” is observed where there are new blood vessels and fibrous connective tissue seen under microscopic examination(2). Targeting this process of abnormal blood vessel proliferation and the fibrous reaction to the tendon injury are the basis of emerging therapies.
The diagnosis of lateral epicondylitis is primarily a clinical one, with a limited role for imaging. Clinically, the patient will present with lateral (outer) elbow pain, sometimes poorly localized and often radiating to the forearm, worse after using the arm for heavy lifting or high demand tasks such as gardening, golfing, or tennis. There is tenderness (pain to the touch) at the lateral epicondyle and characteristic pain with provocation of the wrist extensors.
Radiographs have a limited role but may be useful in more severe cases to exclude contributory abnormalities, including bone deformities, osteoarthritis, loose bodies, or the presence of implants from prior surgery. Radiographs are used as a primary test in someone presenting after an acute injury, as it is important to rule out fractures and dislocations (instability). MRI can be used in select cases after failure of prior treatment to assess the severity of tendon injury. MRI will characteristically demonstrate signal and sometimes tearing within the lateral extensor tendon at the bony origin. MRI can also be used to rule out coexistent injuries, such as to the lateral ligaments of the elbow, when surgery is being contemplated as definitive management.
Once a diagnosis of lateral epicondylitis has been reached, treatment initially consists of activity modification, where potentially inciting activities are discussed and recommendations made to cease or change activities contributing to the problem. There are unproven theories that changing stroke mechanics for the tennis and golf player and using a balanced weight, larger grip club/racquet may improve the condition for some.
Counterforce bracing is also a good option for the active patient wishing to resume activities despite mild symptoms. The strategy of this brace is to squeeze the forearm and extensor tendon at a location just distal (past) the pain source so that less tension (pull) is applied to the area of injury where the tendon attaches to the bone. Some patients prefer a simple compression sleeve, which anecdotally may improve symptoms.

Physical/occupational therapy for eccentric exercise of the elbow muscles, including stretching and modalities have proven effective for many patients(3). Eccentric exercises refer to the application of a load to a muscle as it is lengthening, which can be challenging to do for many patients without the direction of a skilled therapist.
Antiinflammatory treatments, including in pill or local cream form may also be attempted for short-term improvements. Local corticosteroid (“cortisone”) injections may provide anti-inflammatory relief for a short period of time and are typically the most predictable management option for patients with severe symptoms and those in search of at least temporary improvement in pain(4). The pain relief from corticosteroid injections is usually only temporary, so this intervention is most appropriately part of a long-term management plan including exercises/therapy and activity modifications. The risks of these injections include pain flare in the days immediately following injection (before the medication takes full effect) and potentially toxicity to the tendon with repeated exposures.
Platelet rich plasma (PRP) is another experimental injection product that is very safe yet has limited evidence of efficacy. PRP is a natural component of the patient’s blood that when activated, releases high concentrations of anti-inflammatory growth factors that stimulate tissue repair. Studies are ongoing to determine the optimal candidates for PRP injection.
Surgery for lateral epicondylitis is recommended when all other therapies fail and continued pain and disability persists. Surgery involves physically resecting the pathologic angiofibroblastic tissue and is typically done in an “open” fashion where an incision an inch or two long on the outer part of the elbow is used. This is typically considered definitive treatment and successful (5) but should only be used as a last resort. Another less invasive option with mixed results is an ultrasound-guided tenotomy where a needle is used to debride (clean/remove) the abnormal tissue and generate a healing response. These procedures are done on an outpatient basis, where the patient goes home the same day.
Schedule an orthopedic appointment
If you have symptoms consistent with lateral epicondylitis, call our office or book an appointment with elbow surgeon Dr. Thomas Obermeyer. Dr. Obermeyer specializes in diagnosing and treating lateral epicondylitis. Dr. Obermeyer has orthopedic offices in Schaumburg, Bartlett, and Elk Grove Village, Illinois. Dr. Obermeyer regularly sees patients from throughout Illinois including Hoffman Estates, Palatine, Elgin, Streamwood, Arlington Heights, and Roselle communities.
- Nirschl RP. The etiology and treatment of tennis elbow. J Sports Med. 1974 Nov-Dec;2(6):308-23. doi: 10.1177/036354657400200602. PMID: 4468351.
- Nirschl RP. Elbow tendinosis/tennis elbow. Clin Sports Med. 1992 Oct;11(4):851-70. PMID: 1423702.
- Croisier JL, Foidart-Dessalle M, Tinant F, Crielaard JM, Forthomme B. An isokinetic eccentric programme for the management of chronic lateral epicondylar tendinopathy. Br J Sports Med. 2007 Apr;41(4):269-75. doi: 10.1136/bjsm.2006.033324. Epub 2007 Jan 15. PMID: 17224433; PMCID: PMC2658962.
- Tonks JH, Pai SK, Murali SR. Steroid injection therapy is the best conservative treatment for lateral epicondylitis: a prospective randomised controlled trial. Int J Clin Pract. 2007 Feb;61(2):240-6. doi: 10.1111/j.1742-1241.2006.01140.x. PMID: 17166184.
- Nirschl RP, Pettrone FA. Tennis elbow. The surgical treatment of lateral epicondylitis. J Bone Joint Surg Am. 1979 Sep;61(6A):832-9. PMID: 479229.
At a Glance
Dr. Thomas Obermeyer
- 15+ years of training and experience treating complex shoulder and sports medicine conditions
- Expert subspecialized and board-certified orthopedic care
- Award-winning outstanding patient satisfaction scores
- Learn more
