Patellofemoral Pain
Patellofemoral pain is a commonly encountered overuse disorder that involves the front of the knee. The knee can be thought of in terms of three separate compartments, each with different problems that affect them. Two compartments are formed from the mating of the femur (thigh bone) and the tibia (shin bone), where weight is transmitted, and the third compartment formed where the femur mates with the kneecap (patella). It is the latter compartment (patellofemoral) joint that is the focus here. Patellofemoral pain is characterized by pain around or behind the patella that is aggravated by one or more activities that involve loading the patellofemoral joint during activities.
The terminology used to describe patellofemoral pain is used inconsistently and can be confusing. Common alternative terms used include runner’s knee and chondromalacia patella. Chondromalacia patella refers to a distinct pathologic diagnosis that requires advanced imaging and inspection of the cartilage of the area, and while present in some patients with patellofemoral pain, is not required for the diagnosis. Patellofemoral pain is commonly seen in active patients and is slightly more common among women than men(1).
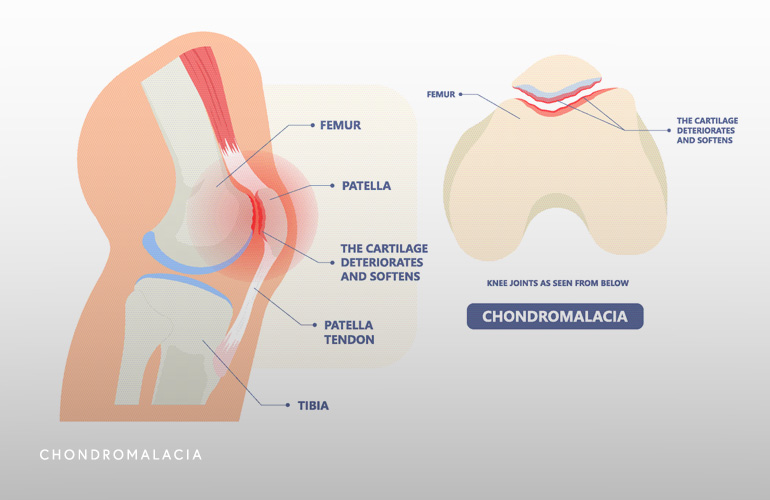
An understanding of the anatomy of the patellofemoral joint is important to understand the causes of patellofemoral pain. The patella bone sits within the quadriceps tendon and rides back and forth in a slot in the femur called the trochlea. The primary function of the patella is to improve leverage of the muscles for knee extension. A common theory known as “patellar tracking” suggests pain develops in this area because of abnormal force generation and distribution during movement of the patella within the trochlea. These tracking problems lead to irritation of the cartilage lining and surrounding tissues with overuse. While the cartilage lining tissue may be one pain generator, the extent of cartilage injury doesn’t always correlate with pain. In other words, sometimes minimal or no cartilage injury can lead to more severe forms of pain. It is for this reason it is believed other structural source of pain include the bone under the cartilage (“subchondral”), lining tissues (called the retinaculum and synovium, and nerves(2).
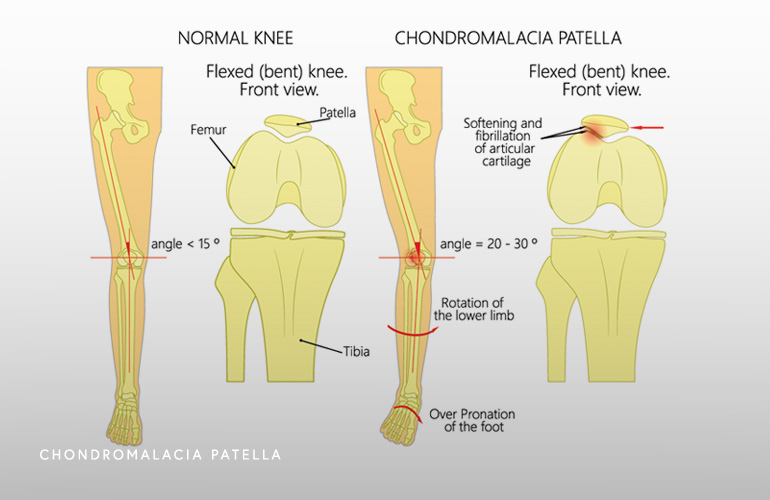
Patellar tracking abnormalities have several potential underlying sources and may relate to not only knee muscle strength irregularities but weakness in the hip abductors and changes in the pronation angle of the foot. It has been shown that runners that under-pronate the foot with heel strike may be at risk of developing patellofemoral pain(3).
Patellofemoral pain typically causes pain that is either anterior (front), lateral (outside), or poorly localized in the knee. While pain is more frequently gradual with overuse, it may also be acute or a result of a traumatic injury. Pain may occur in one or both knees, further supporting the notion there may be structural and anatomic variables contributing to the onset of the condition. Typically pain worsens with squatting, running, prolonged sitting, ascending or descending steps. Pain is commonly described as “achy” but may be “sharp”. Some patients may endorse “giving way” or “buckling” which should be differentiated from other structural disorders causing those symptoms. It is believed that in the setting of patellofemoral pain, these instability symptoms may be due to pain inhibiting proper contraction of the quadriceps. Notably absent in patellofemoral pain is true locking or effusion (swelling within the joint), which are caused by other internal knee problems.
While most of the information on diagnosis of patellofemoral pain is based on clinical factors, imaging can be helpful in the assessment. Radiographs can be used as a screening tool to rule out asymmetry of the position of the patella in the trochlea, developmental changes in the trochlea (called dysplasia) or patella (called bipartite patella), cartilage injuries (called osteochondral lesions), loose bodies, and osteoarthritis. MRI is not typically indicated during the early stages of treatment of patellofemoral pain but if performed can be useful to look for chondromalacia (cartilage injury), osteoarthritis, and other coexistent problems in the peripatellar tissues (including in Hoffa’s fat pad).
In comparison with many other structural knee diagnoses, patellofemoral pain is more commonly treated nonsurgically. The initial treatment of patellofemoral pain involves reducing pain, improving patellar tracking and alignment, and finally to return the patient to as high a level of function as possible.
The initial treatment in the acute phase involves modifying activities that cause pain during rehabilitation. In runners, that may mean reducing or stopping running activities. Athletes may consider alternative aerobic exercises such as bicycle riding, swimming, or elliptical use. Icing and nonsteroidal anti-inflammatory drugs may improve symptoms.
The recovery phase of treatment for patellofemoral pain consists of a structured rehabilitative exercise program, and commonly under the direction of a physical therapist. The combination of knee and hip exercises are employed to increase strength, mobility, and function of the leg. Hip abductor strengthening, core stabilization exercises, and quadriceps strengthening with the foot in a planted position (“closed kinetic chain”) are frequently performed. With these exercises, improvements in patellar tracking if often observed and the pain improves. Sometimes adjuvant treatments including patellar taping, foot orthotics, and other modalities (such as ultrasound, electrical stimulation, among others) may be indicated. In severe or refractory cases, corticosteroid or platelet rich plasma injection may be helpful for temporary relief. As noted previously, surgery for patellofemoral pain is typically avoided and only contemplated in the setting of correctible structural abnormalities diagnosed on imaging.
Schedule an orthopedic appointment
If you have symptoms consistent with patellofemoral pain, call our office or book an appointment with knee surgeon Dr. Thomas Obermeyer. Dr. Obermeyer specializes in diagnosing and treating patellofemoral pain. Dr. Obermeyer has orthopedic offices in Schaumburg, Bartlett, and Elk Grove Village, Illinois. Dr. Obermeyer regularly sees patients from throughout Illinois including Hoffman Estates, Palatine, Elgin, Streamwood, Arlington Heights, and Roselle communities.
- Taunton JE, Ryan MB, Clement DB, McKenzie DC, Lloyd-Smith DR, Zumbo BD. A retrospective case-control analysis of 2002 running injuries. Br J Sports Med. 2002 Apr;36(2):95-101. doi: 10.1136/bjsm.36.2.95. PMID: 11916889; PMCID: PMC1724490.
- Fulkerson JP. Diagnosis and treatment of patients with patellofemoral pain. Am J Sports Med. 2002 May-Jun;30(3):447-56. doi: 10.1177/03635465020300032501. PMID: 12016090.
- Thijs Y, Van Tiggelen D, Roosen P, De Clercq D, Witvrouw E. A prospective study on gait-related intrinsic risk factors for patellofemoral pain. Clin J Sport Med. 2007 Nov;17(6):437-45. doi: 10.1097/JSM.0b013e31815ac44f. PMID: 17993785.
At a Glance
Dr. Thomas Obermeyer
- 15+ years of training and experience treating complex shoulder and sports medicine conditions
- Expert subspecialized and board-certified orthopedic care
- Award-winning outstanding patient satisfaction scores
- Learn more
