Meniscus Tear
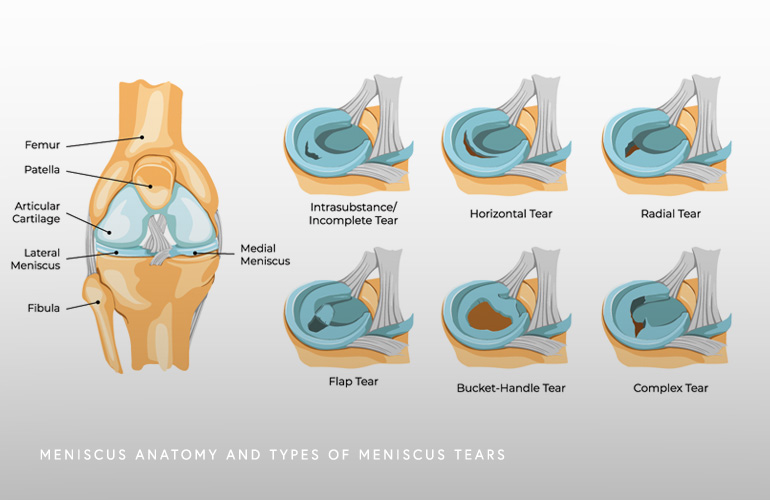
The meniscus of the knee is an important tissue that functions to dissipate loads, stabilize the knee joint during motion, and lubricate the moving surfaces. Because of the location of the meniscus which acts like a “cushion” between the bones, it is susceptible to common forms of injury.
Meniscus Tears in the knee are common. Twisting injuries of the knee can injure a normal meniscus, as can occur with a sporting activity, a lifting event, or a fall. Tears that are more chronic in nature can occur in a meniscus that has a certain degree of degeneration with a more minimal twisting or stress. There are different ways of describing tears in the meniscus, including the side of the knee (medial or lateral), and the morphology including partial or complex, horizontal, vertical, radial, or other types.
Without treatment, meniscus tears can impair the normal smooth back and forth motion of the knee, causing pain, catching, locking, and swelling called an effusion. While meniscus injuries can occur in isolation, they frequently can accompany other associated abnormalities in the knee. These associated abnormalities can occur in the articular cartilage lining of the knee; during more severe injuries, meniscus tears can accompany tears to the collateral or cruciate ligaments. Diagnosing the associated injuries with meniscus tears is important as it can impact treatment and outcome.
Acute tears of the meniscus typically occur when a person changes direction in a way that involves rotating or twisting the knee while the knee is in a slight bent or fully bent posture. Sometimes meniscus tears can occur during a loading event as during a fall, or during activities involving the knee in a flexed position, as when kneeling or when rising from a position on the ground.
Sometimes the meniscus undergoes degeneration or “wear and tear” with age, which does not typically cause symptoms. This process can lower the threshold for injury and sometimes a more minor event can be the cause of a meniscus tear.
The symptoms of a meniscus tear can be variable, as pain and swelling may not be immediately evident. Some patients will describe a tearing or popping sensation at the time of injury, but not always. Most patients can continue with activities or finish out a sporting event that caused the injury with minimal discomfort. Only in severe cases will the knee immediately lock and prevent normal motion and complicate weightbearing. The pain and swelling typically increase over the ensuing 24 hours in a gradual fashion and may come with increased difficulty bearing weight.
Patients with a delay to evaluation with meniscus tears sometimes present for evaluation weeks after an injury with ongoing pain, giving way, catching, or locking in the knee. Most of these symptoms are accompanied by pain because the damaged meniscus is getting impinged or stuck in the joint, limiting normal smooth gliding motion. While “locking and catching” in the knee is traditionally ascribed to meniscus tears, this can also be caused by injury to the articular cartilage lining tissue in the knee and a formal evaluation, sometimes with MRI, is necessary to completely appreciate the extent of the damage.
Another common symptom from a meniscus tear is swelling, called an “effusion” when it is confined to the joint. While not universally present, effusions can be seen with large or complex tears and are usually seen with more substantial injuries to the meniscus. Sometimes effusions are simply described as stiffness (rather than swelling) because the inflated and swollen joint loses some of its normal elastic properties that make it feel as though motion is lost.
Plain radiographs of the are important as an initial screening tool for suspected meniscus injury. These images help to understand whether there is any preexistent osteoarthritis in the knee, which is seen as narrowing of the spaces in the joint when bearing weight, as well as to inspect the bones for injuries to the cartilage lining, to identify calcified or bony loose bodies, and to detect fractures in the setting of an acute injury.
MRI is considered the gold standard for diagnosis, and it can identify the extent and type of meniscus tear. On the initial evaluation, even if a tear is suspected, MRI is not universally required but is often helpful to define the extent of the injury if a more severe tear is present. Because of the high sensitivity at detecting not only meniscus tears but associated injuries, MRI can often help to identify which patients may benefit from arthroscopic surgery and what the long term prognosis for the knee is.
In cases where the knee has good motion, weightbearing is possible, and the knee is not grossly unstable, an initial trial of conservative treatment including rest, elevation, ice, and protection of activities can be helpful. Physical therapy can be helpful to improve the strength of the quadriceps muscles and the overall strength of the leg, particularly when there are findings of degeneration on imaging(1). In the setting of degeneration, steroid injection is sometimes useful for temporary improvement. If the initial conservative approach is unsatisfactory after several weeks or when the tear is caused by a more traumatic event, arthroscopic surgery may be indicated.
Arthroscopic surgery where the knee is inspected with a camera and the torn/damaged tissue is probed and manipulated will provide confirmatory information about the tear and associated injuries. Some tears may be repaired, where the tissue is sutured together to permit healing, while in other cases the torn tissue is conservatively trimmed, so the damaged tissue is removed, resolving symptoms. The decision to repair versus trim (“partial meniscectomy”) is often decided at surgery, as MRI is limited in determining this(2). While partial meniscectomy is more commonly performed than repair, the decision to repair a meniscus depends on the patient’s age, coexistent injuries and status of the cartilage, and the ability to participate in a more involved rehabilitative protocol with more protection of activities for a few weeks. Partial meniscectomy typically has a relatively quick and uncomplicated recovery process where patients are back to most or all of their activities in a couple weeks, with improvements sustained for the ensuing several months after surgery.
Schedule an orthopedic appointment
Are you or a loved one suffering from a meniscus tear? Call or make an appointment online with knee surgeon Dr. Thomas Obermeyer. Dr. Obermeyer is widely regarded as one of the best knee surgeons in Illinois. Dr. Obermeyer has orthopedic offices in Schaumburg, Bartlett, and Elk Grove Village, Illinois. Dr. Obermeyer regularly sees patients from throughout Illinois including Hoffman Estates, Palatine, Elgin, Streamwood, Arlington Heights, and Roselle communities.
- Hohmann E, Glatt V, Tetsworth K, Cote M. Arthroscopic Partial Meniscectomy Versus Physical Therapy for Degenerative Meniscus Lesions: How Robust Is the Current Evidence? A Critical Systematic Review and Qualitative Synthesis. Arthroscopy. 2018 Sep;34(9):2699-2708. doi: 10.1016/j.arthro.2018.04.018. Epub 2018 Jul 20. PMID: 30037571.
- Van der Wal RJ, Ottevanger JW, de Rooij TP, Thomassen BJ, Van Arkel ER. Intraobserver and Interobserver Agreement of Magnetic Resonance Imaging for Reparability of Peripheral Meniscal Tears: What Criteria Really Matter? J Knee Surg. 2017 Mar;30(3):276-282. doi: 10.1055/s-0036-1584536. Epub 2016 Jul 1. PMID: 27367206.
At a Glance
Dr. Thomas Obermeyer
- 15+ years of training and experience treating complex shoulder and sports medicine conditions
- Expert subspecialized and board-certified orthopedic care
- Award-winning outstanding patient satisfaction scores
- Learn more
